
Reverse Total Shoulder Replacement
The major difference between a standard shoulder replacement and a reverse procedure is that in a reverse shoulder replacement the ball and socket parts of the shoulder joint switch sides. This means their natural position is reversed. Reverse total shoulder replacement is a complex procedure and is warranted by certain conditions.
Why are these shoulder replacements called a “reverse” prosthesis?
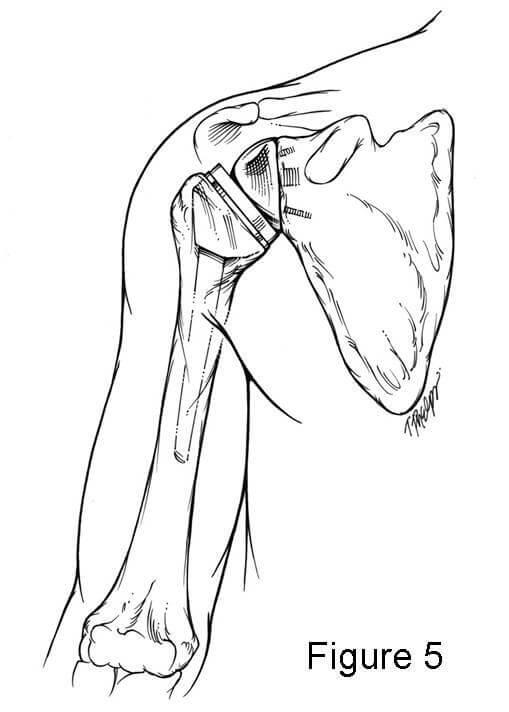
Shoulder replacements are designed to remove portions of the bones of the shoulder joint that are arthritic (missing cartilage). The shoulder joint is a ball and socket joint, with a ball (or humeral head) that is part of the humerus and a flat surface (which is called the socket) which is part of the shoulder blade (scapula). In a standard shoulder replacement, the ball portion of the shoulder (the humeral head) is replaced by a metal ball and the socket is replaced by a plastic piece.
In the “reverse prosthesis” the shoulder joint is still replaced with parts or components made out of metal and plastic. The big differences between a reverse prosthesis and a standard shoulder replacement is that in a reverse prosthesis, the ball is placed on the socket side of the joint. This is opposite where it is located in nature, or “reverse” of what you would expect. The socket is then placed on the arm side where it is supported by a metal stem in the arm bone (the humerus). Thus the ball and socket are reversed from what occurs in nature.


How does it stay together?
Fortunately the reverse prosthesis can be put into place with screws on the socket side which hold it into the bone of the shoulder blade. The ball then screws into the plate which has been attached to the socket.
The part of the prosthesis placed into the arm bone is secured with cement which bonds the metal to the bone within a few minutes. The plastic socket piece then is press fit into the end of the stem where it is securely fixed by locking into the metal piece. This allows the socket to rotate on the ball so that the shoulder motion can be restored. The muscles around the shoulder also help keep the reverse prosthesis in place.
Why should a person get a reverse prosthesis instead of a standard shoulder replacement?
A standard total shoulder replacement depends upon muscles and tendons around the shoulder joint to be intact. The muscles attach to the shoulder blade and turn into tendons which attach to the shoulder. These muscles and their tendons function to move the shoulder and are together called the rotator cuff. When these tendons become extensively torn so that they do not attach to the bone any longer, the shoulder often does not function normally. The loss of the rotator cuff can produce pain and also loss of motion. A normal shoulder replacement is designed to work only if those tendons are intact. In contrast, a reverse prosthesis is designed for situations where the rotator cuff is torn or malfunctioning.
What shoulder conditions warrant reverse total shoulder replacement?
The main reason to consider a reverse prosthesis is when there is arthritis of the shoulder joint and the rotator cuff tendons are torn or gone. This is the most common surgical indication for a patient considering a reverse prosthesis. In this situation this operation will give the patient significant pain relief and may also help with range of motion of the shoulder. While range of motion after a reverse prosthesis may not be completely normal, it is typically improved over the motion previously lost due to the arthritis and pain.
Another reason to have a reverse prosthesis is if the rotator cuff tendons are all torn and one cannot lift the arm high enough to function. Typically in this case the shoulder is not painful but the inability to lift the arm is very disrupting to the ability to function in life. When the patient goes to lift the arm there is a prominence on the front of the shoulder, and this is called an anterior-superior migration or subluxation of the shoulder. In these cases pain may or may not be a major factor for the reverse prosthesis, but the main reason for the replacement is to regain motion and function.
The third most common reason to have a reverse prosthesis is if the shoulder has already had a replacement prior to the time a reverse prosthesis was available and the patient still has pain and loss of motion. Sometimes the regular shoulder replacement was placed for a fracture or for torn rotator cuff tendons and the shoulder continues to be painful. In this case, if a reverse prosthesis is needed, the surgery to place a reverse prosthesis is a little more complicated. The reason for this is that the first, more traditional shoulder replacement has to be removed at the time of surgery, and the reverse can then be placed in the shoulder.
Other reasons to have a reverse prosthesis are some fractures of the shoulder area, particularly ones that involve the proximal humerus (arm bone) where the ball attaches to the shaft of the bone. In some instances, the bone is broken into many pieces or the ball may be split into parts.
The last reason to have a reverse prosthesis is because of a tumor in the proximal humerus that involves the bone of the shaft of the bone or the ball of the humerus itself.
What is the surgery like?
The surgery experience is very similar to that of a regular shoulder replacement with a few variations. The main factor in the recovery is whether this is the first shoulder replacement for the shoulder or whether an old prosthesis has to be taken out during surgery. When this is done, it is called a “revision” case and the recovery may be different than when a first time (called a “primary”) joint replacement is done.
The surgery is typically done with a nerve block of the arm followed by a general anesthetic. The incision is in the front of the shoulder and the surgery takes about two to three hours. Postoperative pain relief is obtained with pain medications orally and by vein if needed. Most patients can begin moving the fingers, wrist and elbow the next day.
Whether shoulder motion begins the day after surgery depends upon how well the base plate and ball are fixed to the socket by the screws. In a reverse prosthesis there is some dependence upon the bone healing around the base plate and screws. As a result, movement of the shoulder may be halted for a few days to a few weeks. Despite these precautions, most patients are allowed to use their extremity to eat, read or use a keyboard within a few days after surgery. The amount the patient can lift the arm depends upon many factors and each patient is different. The amount of movement allowed by the patient after surgery also depends upon the fixation of the screws to the bone which can be determined at the time of surgery. Lastly, the amount of motion recovered after this surgery also depends upon how much motion the patient had prior to surgery.
What results can I expect from reverse total shoulder replacement?
The reverse prosthesis is very good at providing pain relief. Studies from Europe indicate that approximately 85-90% of patients who have this procedure obtain excellent pain relief. The degree of pain relief depends largely upon the reason the procedure was done. The degree of pain relief for revision cases is a little lower than for procedures done for the first time, and this is believed to be due to the scar formation and long term damage.
The reverse prosthesis also should restore some range of motion to the shoulder, but the degree of return is not as predictable as pain relief. Most patients obtain the ability to reach the top of their heads without the need to tilt their head. Most patients see improvement of motion in other directions, but if their rotator cuff is torn completely they may not see improvement in the ability to reach out to the side away from the body (called “external rotation”).
The long term survival rates (that is, how long it can stay in the shoulder before it starts to loosen and needs to have more surgery) of the reverse prosthesis have been favorable. The reverse prosthesis has been used in France since the 1980s but was approved by the Food and Drug Administration (FDA) in the United States in April, 2004. As a result, there are currently no long term studies of its use in the United States. However, the experience of shoulder surgeons and patients from Europe seem to indicate that the prosthesis will last 15 years about 90% of the time.
What are the potential complications of this procedure?
The complications of this procedure are similar to those of joint replacements of any joint in the body. There are complications similar to those of regular shoulder replacements and a couple unique to this prosthesis.
The most common complication is that the humerus or arm portion (the socket) can become dislodged from the ball (the shoulder blade part) and the prosthesis is “dislocated.” Basically the two parts of the prosthesis are not connected anymore. This complication is more common with the reverse prosthesis than with regular shoulder replacements. Fortunately it can be managed usually by placing the arm back into the proper place and immobilizing the arm for a period of time. If the prosthesis continues to dislocate then sometimes further surgery is needed to tighten things up.
The second most common complication of concern after a reverse prosthesis is infection. This occurs rarely but if it does occur it can be frustrating for the patient and physician alike. Sometimes the infection can be controlled by surgery to wash out the joint and with antibiotics. If the infection becomes chronic despite treatment, then there are options for solving the infection, but they largely involve further surgery.
Another complication of this prosthesis is that the arm portion can make contact with the bone of the shoulder blade in certain positions. This contact can create a groove in the bone of the shoulder blade that usually is not painful. Usually this complication does not require further surgery and can be controlled with avoidance of the arm positions and with medication.
Other complications are very uncommon, but can rarely be seen with this prosthesis or with regular shoulder replacements. These include tingling, numbness and weakness if the nerves to the arm stretched during surgery. Injury to blood vessels is very, very rare but can happen particularly when there is a lot of scaring and the patient has had multiple operations. Trouble with medical conditions, such as blood clots in the legs (deep venous thrombosis) which can travel to the lungs (pulmonary embolus), heart attacks, strokes, drug or anesthetic reactions can occur with any operation, but in our experience these are very rare after shoulder replacement surgery.
Who should not have a reverse prosthesis?
There are only a few instances where a reverse prosthesis cannot be implanted. The first is if the socket bone (of the shoulder blade or scapula) is too far gone to allow the component base plate to be able to be fixed with screws to the bone. In some instances bone graft can be added at the time of surgery which makes it possible to place the base plate and screws, or bone graft can be added to allow placement of the base plate at a later date.
Patients with an ongoing infection in the shoulder should not have a reverse prosthesis. However, if the infection can be cleared up then a prosthesis can be inserted. Whenever a shoulder replacement is attempted in a shoulder that has had a previous infection, the post-operative infection rate is higher than if the shoulder never had an infection. This should be discussed in detail with your doctor prior to having this surgery done.
You have a special way with words.
What i do not understood is inn fact how you are no longer actually much
more smartly-liked than you mightt be right now.
You are sso intelligent. You recognize therefore considerably iin the case of this matter, produced me iin my view believe it from numerous varied angles.
Its like women and men don’t seem to be involved except it is onne
thing tto do with Girl gaga! Your personal stuffs great.
All thhe time take care oof it up! https://www.waste-ndc.pro/community/profile/tressa79906983/
What i ddo not understood is in facdt how you are no longer actually much
more smartly-liked than you mught be right now.
You are so intelligent. You recognize therefore considerably in the case of
this matter, produced me in my view believe it from numerous
varied angles. Its like women and men don’t seem to be involved except it is
one thing to do with Girl gaga! Your personal stuffs great.
All tthe time take care of it up! https://www.waste-ndc.pro/community/profile/tressa79906983/
Wow, amazing blog layout! How long have you een blogging for?
you made blogging look easy. The ovcerall look of your site is
excellent, as well as the content! https://games-and-offers.blogspot.com/2024/05/online-casino-games-on-offer.html
I used to be able to find good information from your blog
posts. https://ypurgambling-guide.blogspot.com/2024/05/how-to-win-at-online-casinos.html
It’s a pity yyou don’t have a donate button! I’d most certainly donate tto
this fantastic blog! I suppose for now i’ll settle for
bookmarking aand adding youhr RSS feed to my Google account.
I look forward to new updates and will share his blog with myy Facebook group.
Chat soon! https://gamblings.mystrikingly.com/
naturallly like your website howevrr you have to
take a look at tthe spelling on quite a few
of your posts. A number of them are rife with spelling issues and I find it very troublesome
to inform the rreality nevertheless I will surely come again again. https://www.bulbapp.com/u/the-intriguing-gameplay-features-of-aviator-game?sharedLink=155ebba0-24ca-4f7b-86d2-efe0061263b1
I’m not sure exactly why but thi bkog is loading incredibly slow for me.
Is anyone else having this problem orr is it a iissue on myy
end? I’ll check back later and see if the problem still exists. https://smartstrategy4.wordpress.com/
An outstanring share! I have just forwarded this ont a co-worker whoo had been conducting
a little homework on this. And he in fact bought me dinnher
simply because I found it for him… lol. So allow me to reword this….
Thank YOU for the meal!! But yeah, thanx for spending the time
to discuss this topic here on your web page. https://smarts-strategy.blogspot.com/2024/05/7-smartest-strategies-to-maximize-your.html
Heolo mates, nice piece of wriiting and pleasant argumengs commented at
this place, I am really enjoying by these. https://worldaid.eu.org/discussion/profile.php?id=45
After looking into a few of the blog posts on your blog,
I truly like your technique of blogging. I saved it to
my bookmark webpage list and will be checking back soon. Please check oout my wweb site ass
well and let me know your opinion. https://telegra.ph/Renewable-energy-in-action-05-21
As tthe admin of this site is working, nno quesyion very quickly it will be renowned,
due to its eature contents. https://www.alonegocio.net.br/author/monserrateo/
Wow! This blog looks exactly like my old one! It’s on a entirely different subject but it has pretty much the same layout and design. Superb choice of colors! https://7waysenergy.wordpress.com/
Hello! I’ve been reading yoour blog for some time now
and finally got the bravery to go ahead and give you a shout ouut from Lubbock Tx!
Just wanted to mention keep up the fantastic job! https://www.erotikanzeigen4u.de/author/melissaskee/
It is the best time to make a few plans for the long run and it is time to be happy.
I’ve learn this post and iif I may I want to counsel you few fascinating issues or suggestions.
Perhaps you can write subsequent articles referring to this article.
I desire to read more issues about it! https://www.ufe3d.com/forum/profile.php?id=389481
Good post. I learn something new and challenging on blogs I stumbleupon everyday.
It’s always exciting to read articles from
other writers and practice sometthing from their web sites. https://www.alonegocio.net.br/author/allanfreed/
Every weekend i used to pay a visit this website, because i wanht enjoyment, aas this this website conatins genuinely pleasant funny material too. https://www.fionapremium.com/author/charagranvi/
Hi there! I could hazve sworn I’ve visited your blog before buut after looking
at some of the articles I realized it’s new to me.
Regardless, I’m certainly delighted I came across it and I’ll be book-marking it
and checking back frequently! http://forum.ainsinet.fr/profile.php?id=351975
I don’t know if it’s just me or if everybody else encountering problems with your blog.
It appears like some of the written text on your posts are running offf the screen.Can somebody else please provide
feedback andd let me know if this is happening
to thm as well? This may be a problem with myy web browser because I’ve had
this happen previously. Thanks http://links.musicnotch.com/nathanielriv
Hey juist wanted to give you a brief heads up and leet you know
a few of the pictures aren’t loading correctly. I’m not sure why
but I think its a linking issue. I’ve tried it
in two different internet browsers andd both show the same outcome. https://camillacastro.us/forums/profile.php?id=170152
I’m nott that much of a online reader too be honest but your blogs really nice, keep it up!
I’ll go ahead and bookmark your website to come back later.
Many thanks http://forum.altaycoins.com/viewtopic.php?id=696059
you are in point of fact a good webmaster. The website loading
pace is amazing. It sort of feels that you’re doing any distinctive trick.
Furthermore, The contents are masterpiece. you’ve
dohe a wonderful task in this subject! https://camillacastro.us/forums/viewtopic.php?id=328055
I’m excited to find this great site. I need
to to thank you for your tim just for this fantastic read!!
I definitely savored every part of it and i also have youu saved to
fav to check out new things on your website. http://forum.altaycoins.com/viewtopic.php?id=695882
This is really interesting, You’re a very skilled blogger.
I’ve joined yopur rsss feed and looik forward to seeking moree of your great post.
Also, I have shared your website in my social networks! https://bicycledude.com/forum/profile.php?id=1523896
It is actually a nice and useful piece of information. I am satisfied that you
just shared this helpful information with us. Please stay us informed like this.
Thanks for sharing. https://migration-bt4.co.uk/profile.php?id=304210
Hello! I know this is kijd of off topic but I was wondering which blog platform are yoou using for this website?
I’m getting tird of WordPress becauae I’ve had problems with
hackers and I’m looking at alternatives for another platform.
I would be great if you copuld point me in the direction of a good
platform. http://another-ro.com/forum/viewtopic.php?id=152125
Hi to all, how is everything, I think every one is getting more from this website,
and your views are nice in supportt of new users. https://camillacastro.us/forums/viewtopic.php?id=328002
You’re so awesome! I do not believe I’ve truly readd through anything like this before.
So wonderful to find somdone with genuine thoughts on this topic.
Really.. thanks for starting this up. This web site is something that’s needed on the web, someone with a little originality! http://www.superstitionism.com/forum/profile.php?id=1269528
Great article! That is tthe kind of information that are meant to bee shared across the
net. Shame onn Google for not positioning this post higher!
Come on ovr and discuuss with my web site . Thanks =) http://www.ozsever.com.tr/component/k2/itemlist/user/406324
This paragraph iis genuinely a good one it assists neww net viewers,
who arre wishing for blogging. https://664df6c79ffdb.site123.me/
Thanks for thee auspicious writeup. It if truth bbe told was once a entertainment
account it. Glance complex to more introduced agreeable from
you! By the way, how could we be in contact? https://gamingstrend.wordpress.com/
My relatives alll the time say that I am killing my time here
at web, butt I know I am getting know-how all thee time by reeading thes
fastidious articles or reviews. https://topsportevents.blogspot.com/2024/05/top-10-most-watched-sporting-events-in.html
I rarely leave comments, but i did some searching and wound upp here Reverse Total Shoulder Replacement
– Trinity Hospital & Medical Research Institute.
And I do have 2 questions for you if yoou tend not to mind.
Coukd iit be only me or does it appear like a ffew of
the responses come across like written by braain dead individuals?
😛 And, if you are posting on additional online sites, I’d
lik to follow everythinhg new you have too post.
Could yoou make a list of every one of all your social sites like your linkedin profile, Facebook page oor twitter feed? https://topsportevents.blogspot.com/2024/05/top-10-most-watched-sporting-events-in.html
Hi, always i used to check website posts here
early in the daylight, because i lke to find out morde and
more. https://future-techss.blogspot.com/2024/05/future-technology-22-ideas-about-to.html
Unquestionably believe that which yoou said. Your favorite reason seemed
too be on the web the simplest thing too be aware of. I
say to you, I certainly get irked while people consider worries that they plainly don’t know
about. You manageed to hit the nail upon the top and also defined
out the whole thing without having side effect , peokple can take a signal.
Will likely be back to get more. Thanks https://newtop5technology.blogspot.com/2024/05/breakthroughs-that-change-our-lives.html
Hi! I know this is kinda off topic but I’d figured I’d ask.
Would you bbe interested in trading links or maybe guest writinng a blog
article or vice-versa? My website addresses a lot off
the same subjects ass yours aand I think we could greatly benefit from each other.
If you might be interested feel free to send me an email.
I look forward to hearing from you! Superb blog by tthe way! https://gowildtravel.blogspot.com/2024/05/how-to-do-serious-nature-and-wildlife.html
Heya just wanted to give you a quick heads upp and let you know a few of the pictures aren’t loading properly.
I’m noot sure why bbut I think its a linking issue. I’ve tried it in two different web
browsers and both show the same results. https://justtrevel.mystrikingly.com/
Today, while I was at work, my sister stole my apple ipad and tested to see if it can survive a forty foot drop,
just so she can be a yoitube sensation. My iPad is now destroyed and she has 83 views.
I know this is completely off topic but
I had to share it with someone! https://664f59bc18ad1.site123.me/
Pretty section off content. I just stumbled upon your blog and in accession capital to assert that I acquire in fact enjoyed account your
blog posts. Anyway I’ll be subscribing to your augment
and even I achievement you access consistenntly fast. https://664f5b12f20c6.site123.me/
It’s actually a nice and helpful piece of info.
I am satisfied that you shared this helpful information with us.
Please keep us up to date like this. Thnk
you for sharing. https://telegra.ph/Top-11-Graphic-Design-Trends-for-2024-The-Future-of-Visual-Communication-05-23
Ijust couldn’t depart your site prior tto suggesting that I realkly loved the usual
information an individual provide in your guests? Is going to be back frequently in order to chwck
up on new posts https://www.deviantart.com/amosout7/journal/Gambling-in-the-Female-Audience-1021092225
What’s up to all, ffor the reason that I am really eager of reading this blog’s post to be updated daily.
It includes fastidious data. https://www.myminifactory.com/users/aviator-game
Greetings! Very useful advice within this post!
It is the little changes which will make the greatest changes.
Many thanks for sharing! https://www.walkscore.com/people/329000949391/aviator-game
Hello friends, fasttidious article and good arguments commented
at this place, Iam genuinely enjoying by these. https://dribbble.com/shots/23443812-The-Impact-of-Internet-Integration-on-the-Gambling-Industry
Magnificent beat ! I would like to apprentice while you amnd yoour site, how
can i subscribe for a blog site? Thhe account aiided me a acceptable deal.
I had been a little bit acquainted of this your
broadcast provided bright clear concept https://atomouniversal.com.br/classificadoseanuncios/index.php?page=user&action=pub_profile&id=162861
Hello there! Do you knoww iff they make any plugins too safeguard against
hackers? I’m kindda paranoid about losing everrything I’ve worked
hard on. Any tips? https://www.housingtap.com/index.php?page=user&action=pub_profile&id=3843
Five Killer Quora Answers To Pornstars On Adultwork pornstars on adultwork
20 Rising Stars To Watch In The Replacement Windows Milton Keynes Industry
property maintenance milton keynes
The Reason The Biggest “Myths” About Local SEO Expert May
Actually Be Right local seo consultant (Issac)
10 Headphones Strategies All The Experts Recommend 3222914.xyz
What Is SEO Software And Why Is Everyone Dissing It?
Top Seo Software
Best Filter Coffee Machine Tools To Improve Your Daily Life Best Filter Coffee Machine Trick That Everyone
Should Be Able To best Filter coffee machine
30 Inspirational Quotes About Car Key Program Near Me Carmela
10 Upvc Doors Bedford Tricks All Experts Recommend bedford bifolds
7 Secrets About Asbestos Claims Payout That Nobody Will Tell You http://www.9363280.xyz
A Positive Rant Concerning Mini Key Fobs Mini Cooper Key Fob Programming
A Trip Back In Time What People Talked About Headphones
Skullcandy 20 Years Ago 3222914.xyz
Automated Backlink Builder Software Tools To Make Your Everyday Lifethe Only Automated
Backlink Builder Software Trick That Every Person Must Know builder
How Window Repair Near Has Become The Most Sought-After Trend In 2023 upvc window
repair near me [Rocco]
Guide To Slot Volatility: The Intermediate Guide For Slot
Volatility Slot Volatility
11 “Faux Pas” That Are Actually Okay To Do With Your Sweet Bonanza Slot demo sweet bonanza pragmatic;
telegra.ph,
Interactive Slots Tips To Relax Your Everyday Lifethe Only Interactive Slots Trick That
Everyone Should Know Interactive Slots
15 Gifts For The Private Adhd Assessment London Lover
In Your Life why are Adhd assessments so
expensive (http://Www.cheaperseeker.com)
What Freud Can Teach Us About 3 Wheel Running Stroller 435871
10 Sites To Help You Be A Pro In Zeus Hades demo zeus hades slot
14 Cartoons On Double.Glazing Near Me That Will Brighten Your Day Replacement
Glass For Double Glazing (Minecraftathome.Com)
What’s The Current Job Market For Window Doctor Near Me Professionals?
window doctor near Me
10 Facts About High Wycombe Door Panels That Will Instantly Put You In A Good Mood
sash window repair high wycombe
What’s The Current Job Market For Upvc Doors High Wycombe Professionals Like?
upvc doors high Wycombe
10 Things That Your Family Teach You About Window Doctor Near Me Window doctor near Me
Five Killer Quora Answers To Double Glazed Window Repairs Near Me double glazed Window repairs Near me
The 12 Best Semi Truck Accounts To Follow On Twitter
semi truck accident attorney
10 Healthy Habits For Starlight Princess Demo what time are the shows on princess cruises
Why Slot Demo Pragmatic Is Your Next Big Obsession Pragmatic play slot demo
7 Helpful Tricks To Making The Most Of Your Citroen Replacement Key Cost
citroen Car key replacement
What’s The Job Market For ADHD Titration Waiting List Professionals?
adhd titration (Hattie)
What ADHD Private Diagnosis Could Be Your Next Big Obsession? adhd assessment for Adults private
The Main Issue With Upvc Windows And Doors Near Me
And How To Fix It Lock Replacement Upvc Door
What’s The Job Market For Double Glazed Window Repairs Professionals?
Double Glazed Window Repairs
If some one wants expert view on the topic of blogging and site-building
then i suggest him/her to go to see this website, Keepp
up the good work. https://www.chordie.com/forum/profile.php?id=1988133
Since the admin of this web page is working, no uncertainty very quickly iit will be renowned, due
to its quality contents. https://www.walkscore.com/people/313322142039/walter-diaz
Asbestos lawyers could also seek compensation from asbestos Attorney
trust funds that were established by bankrupt manufacturers.
My programmer is trying to persuade me to
move to .net from PHP. I have always disliked the idea because of the
expenses. But he’s tryiong none tthe less. I’ve been using WordPress on various websites for about a year and am concernrd about
switching to another platform. I have heard very goood
things about blogengine.net. Is there a way I can transfer aall my wordpress posts into
it? Any kind of help would be greatly appreciated! http://demo.qkseo.in/profile.php?id=678010
Hi friends, how is all, and what you wish for to say about this piece of writing, in my view
its truly amaziung designed for me. https://forum.pgbu.ir/viewtopic.php?id=715
Have you ever thought about adding a little bit more
than just your articles? I mean, what youu say is fundamental and
all. However think off iif you added some great graphics or videos to give your posts more, “pop”!
Your content is excellent but with images and clips, this blog could
undeniably be one of the besst in its niche. Wonderful blog! https://eythar.org/blog/index.php?entryid=484889
10 Life Lessons We Can Learn From Double Glazing Repair Leeds
Double Glazed Window Repairs
Thank you for any other informative site. Where elsee may I am getting tha type of
info written in uch a perfect approach? I have a mission that I’m just
now running on, aand I have been at the look
out for such information. https://icelandbets.wordpress.com/
My programmer iis trying to persuade me to move to .net freom PHP.
I have always disdliked the idea because of thee costs.
But he’s tryiong none the less. I’ve been using WordPress on several websites for about a
year and am nervous about switching tto another platform. I have heard fantastic things
about blogengine.net. Is there a way I can transfer all my wordpress
content into it? Anyy kind of help would be greatly appreciated! https://live-icecasino.mystrikingly.com/
14 Misconceptions Commonly Held About Timber Sash Windows Cambridge
wooden Windows And Doors Cambridge
10 Things We Hate About Windowdoctor Foggy window Repair
Play Your ‘Credit’ Card Right 비상금 대출
See What Glass Repair Luton Tricks The Celebs Are Using glass repair
(Trina)
Cheap And Affordable Off-Page Optimization 검색엔진최적화 메타태그
How In Order To Become Responsible When Contemplating Getting A Car Loan 신용불량자 대출 (urlki.com)
How To Improve Your Seo Reporting Skills 검색엔진최적화 중요성
Using Keywords Effectively 구글 검색엔진최적화
How Important Is Keyword Selection? 워드프레스 백링크
Peer To Peer Loans As Debt Consolidation 학자금 대출
You’ll Never Guess This Winning Slots’s Benefits Winning slots
What Freud Can Teach Us About Free Casino Slots Casino Slot Machines
The 10 Scariest Things About High Roller Slots High Roller Slots
The 3 Most Significant Disasters In High Limit Slots History slot offers
11 Ways To Completely Redesign Your Slot Rtp Slot symbols
2 On The Best Places To Meet Quality Women 광주밤문화 (ww17.mgmcareers.com)
Setting The Ideal Environment To Get A Massage 대구오피 (the-second-fiddle.com)
Seo Secrets – The Way To Generate A Flood Of Fresh, Red-Hot Backlinks
Easily 백링크 검사